Turkey initiated its Health Transformation Program (HTP) in 2003. Prior to the HTP, its health service delivery was fragmented and relied heavily on the higher cost of hospital care. Primary care was inadequate and trained health workers in short supply and distributed inequitably. Overall, the health sector was underfinanced and governance in it was weak. In time, though, the HTP de-fragmented financing and service delivery, and expanded coverage to nearly the entire population.
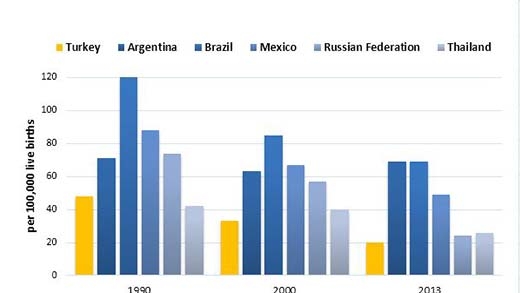
Today, Turkey is often cited as a success story: it has improved its health outcomes, achieving health-related millennium development goals well before the 2015 deadline. The number of women dying from pregnancy-related causes more than halved since 1990 to about 20 per 100,000 live births in 2013. The number of infants dying before their first birthday dropped from 55.7 in 1990 to 16.5 per 1,000 live births in 2012.